Digital dentistry: discover its benefits and how libraries are used

The digital era is here to stay, so much so that the methodology is being increasingly used during tasks, providing us dentists with easier ways of optimising treatments and shortening the time spent on them, as well as being able to work in a more guided and predictable manner.
Digital dentistry use has spread throughout every sector of the profession, for treatment such as orthodontics (digitally guided splints), dental aesthetics (smile designs, wax-up, digitally guided veneers, etc.), prosthesis (fixed onto a natural tooth or implants, and removable), and surgery (both guided and navigated).
Digitalisation offers many advantages over analogue protocols. These include precision when tailoring our tasks, speed and efficiency, both in terms of communication with our laboratory and completing our work, or predictability during work. We already know what we are going to treat in the surgery, and if a design is satisfactory, we can even reproduce it as many times as we want. Not so long ago, manufacturing precisely the same tooth was unthinkable. However, it is now a reality and we can go one step further in terms of copying the tooth on the opposite side of the mouth and reproducing it identically to provide great aesthetic results.
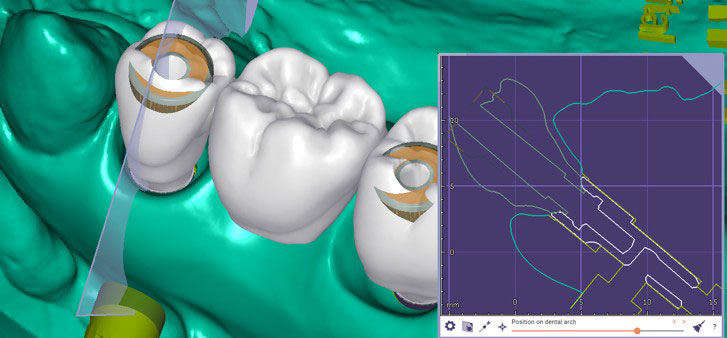
However, as with all disciplines, a dentist needs to learn and undergo a change of mindset, with a basic understanding of analogue procedures essential to better understand the digital equivalent. For example, an impression coping or transfer is required to create an analogue prosthesis for an implant. In digital terminology, this may be called a Scan Abutment or Scanbody. Each Scanbody (specific to a particular type of implant) has a specific digital library (each brand has their own). This provides access to the different prosthetic solutions available for that implant, perfectly correlated in three dimensions (the x, y, z axes).
The significant financial outlay required at the outset of digital dentistry was undoubtedly one of the major disadvantages, as each brand sold their own Scan Abutments and their libraries to both the clinic and its laboratory. This led to working with only one or two brands of implants to avoid raising costs too high, limiting potential solutions for different problems.
However, in time, companies like IPD provided a solution to these drawbacks, providing Scanbodies that are compatible with most implant brands and a high quality level during manufacturing. For example, they ensured manufacturing tolerances of 5 microns, guaranteeing the necessary precision to undertake a task correctly. In order to complete the required digital flow, IPD provides an extensive range of libraries (free of charge), which means we have multiple solutions to hand without needing to have many tools in stock.
In practical terms, the digital solution can be separated into 3 main parts: SCANBODY + PROSTHETIC SOLUTION + DIGITAL ANALOGUE
There are many types of Scanbodies (PEEK, PEEK with a metal base, metal only, engaging or non-engaging, etc.). These are chosen based on requirements and come with their own libraries. Using Scanbodies with a titanium base makes X-raying to check the seal with the implant easier. Its durability as a component for everyday use is another advantage, while the upper section in PEEK helps to obtain a better scanner reading avoiding too much light and oversizing.
Not many brands currently offer interfaces with an emergence profile over 1 mm, and as pointed out by the studies from Linkevicius T. et al, 2009, and Galindo-Moreno et al, 2014, among others, keeping the prosthetic connection as far away as possible from the implant head is essential. There is a significantly higher level of bone loss from the ridge with implants restored with short abutments (<2mm) compared to when using abutments >2mm.
Available up to 3.5 mm in height, being able to choose different emergence profiles is important when it comes to meeting any need during work undertaken involving soft tissue.
IPD has found an answer for both this type of case and restorations by using an interface. They have designed them to provide a cementing height of up to 8 mm, meaning they can be cut at different levels, using a guide that the technician can choose based on requirements, and they can even prepare a window to modify the emergence of the prosthetic screw channel.
Along with digital training support, being supported by a department specialised in CADCAM makes working throughout the digital flow easier, providing a simpler introduction to digitalisation.
To sum up, the decisive factors when it comes to choosing from the multiple Scanbodies available in the market should not be limited to quality and fit, which come as standard in most options, but having open libraries available that offer many restoration options, providing an answer to every possible clinical need (using an interface, over the epithelium, direct to implant, 3D analogue, etc.).
As such and before deciding, it is worth looking into which one offers the most complete prosthetic solutions and suitable digital support.